Received: Mon 05, Feb 2024
Accepted: Tue 20, Feb 2024
Abstract
Although phytochemicals are plant-derived toxins that are primarily produced by plants as a form of defense against insects or microbes, several lines of studies have demonstrated that phytochemicals (e.g., polyphenols, carotenoids, and amino acids) have several beneficial biological actions for human health, such as anti-oxidative, anti-inflammatory, and cardioprotective effects. Recent studies have demonstrated that phytochemicals can modulate neuronal excitability in the nervous system, including nociceptive sensory transmission, so it is possible that phytochemicals could be complementary alternative medicine candidates; specifically, therapeutic agents against pain. The focus of this review is to elucidate the mechanisms underlying the modulatory effects of phytochemicals on neuronal electrical signals, such as generator potentials, action potentials, and postsynaptic potentials, in the nociceptive pathway neurons resulting in potential local anesthetic effects, intravenous anesthesia and analgesic effects, and inflammatory pain relief effects. In addition, we discuss the contribution of phytochemicals to the relief of nociceptive and/or pathological pain and their potential clinical application on the basis of our recent studies in vivo.
Keywords
Phytochemical, complementary alternative medicine, nociception, pathological pain, neurophysiology, electrophysiology, anesthesia, inflammation
Highlights
• Phytochemicals modulate neuronal excitability of nociceptive pathway neurons.
• Local application of phytochemicals into the receptive field suppresses nociceptive neurons.
• Intravenous application of phytochemicals inhibits nociceptive neurons via the descending inhibitory system.
• Systemic administration of phytochemicals attenuates inflammatory hyperalgesia.
• Phytochemicals are potential complementary alternative medicines for the treatment of pain.
1. Introduction
Recently, complementary alternative medicine (CAM) has been actively used for patients with symptoms for whom western medical treatment, such as drug therapy, does not work, and CAM is expected to be useful in the treatment of chronic pain [1-3]. CAM is defined by current western medicine as a medical system that has not been scientifically tested and clinically applied. In general, CAM is known mainly for herbal medicines and acupuncture. Phytochemicals are plant-derived toxins, primarily produced by plants as a form of defense against insects or microbes. However, some plant-derived chemical components, such as phytochemicals contained in foods, have various beneficial biological functions, such as anti-cancer, anti-oxidant, anti-arteriosclerotic, and blood pressure-lowering effects [4, 5].
The main phytochemicals include the various natural products derived from vegetables and fruits, such as polyphenols (resveratrol, chlorogenic acid, isoflavone, catechin, and quercetin), carotenoids (lutein), and amino acids (theanine). Polyphenols comprise a large variety of molecules amongst which some have a unique phenol ring (phenolic acids, phenolic alcohols) or typically more than one phenol ring. Depending on the number of phenol rings and the structural elements binding these rings together, polyphenols are divided into different groups, as follows; flavonoids (chlorogenic acid, isoflavone, catechin, quercetin), phenolic acids, phenolic alcohols, stilbene (resveratrol) and lignans [6, 7]. For example, resveratrol is contained in grape seeds and skins, chlorogenic acid is contained in coffee beans, isoflavones are found in soybeans, quercetin is found in onions, and catechin is found in green teas. Lutein is a naturally occurring carotenoid present in fruits and leafy vegetables [8]. Theanine (γ-glutamylethylamide) is an amino acid derived from glutamic acid and found almost exclusively in certain teas.
In recent years, the functions of phytochemicals have attracted attention as chemical components of foods for specified health uses, and in foods with claims of preventing lifestyle diseases [4, 5]. In general, drugs used to treat diseases have side effects as well as their main action aimed at relieving symptoms, but many of the phytochemical components derived from food do not have clear side effects [4, 5]. Therefore, it is presumed that using phytochemical components of foods as CAM is of great importance for the development of highly safe treatment methods that do not rely on drugs.
Recent studies demonstrated that these phytochemicals can modulate the generation of neuronal electrical signals, such as generator potentials, action potentials, and postsynaptic potentials, in neurons, including nociceptive neurons, in the central nervous system (CNS) and peripheral nervous system of mammals. Modulation of ligand-gated ion channel currents and neurotransmitter/receptor function by phytochemicals has been reported mainly under in vitro experimental conditions [9-19]. Based on these in vitro experimental findings, we recently studied the pain-relieving effects of phytochemical components contained in foods using a neurophysiological approach based on animal experiments in our laboratory, and have published studies on the following effects of these phytochemicals: (i) potential local anesthetic effects; (ii) intravenous anesthesia and analgesic effects; and (ii) inflammatory pain relief effects. In this review, we discuss the contribution of phytochemicals to the relief of nociceptive and/or pathological pain and its potential clinical application on the basis of our recent in vivo studies.
2. Classification of Pain
Congenital analgesia is a genetic disease in which nociceptors are deficient [20]. Since patients with congenital analgesia do not feel pain, their joints are deformed by repeated fractures, and they are often subjected to fatal disabilities, such as tissue necrosis and sepsis from burns, and are always in danger of their life. This highlights that pain is a "biological warning signal" to protect the body from tissue damage caused by nociceptive stimuli applied to the body, and is a sensation that is essential for our survival [21]. Pain that generally acts as a warning signal is called physiological pain, or nociceptive pain. On the other hand, there is pain that no longer serves as a "biological warning signal." This is “pathological pain” in which there are changes in the nature of the neurons that form the pain transmission pathway and the continuous activation of signal transduction provides pain to the body, significantly impairing the quality of life, even if substantial tissue damage has disappeared or repaired [21].
Pathological pain is pain that no longer serves as a warning signal; for example, inflammatory pain or neuropathic pain. Inflammatory pain is pain caused by the sensitization of nociceptors by inflammatory chemicals (e.g., prostaglandin E2 [PGE2]) at the site of tissue damage, such as burns and joint pain [22]. Neuropathic pain is caused by nerve damage and continues to be painful, even after the injury has healed, such as with tooth extractions and implants in clinical dentistry. The main neuropathic pains are diabetic neuropathy, sciatica, and trigeminal neuralgia. Common symptoms of these pathological pains include hyperalgesia and allodynia [23, 24]. Hyperalgesia is increased sensitivity to pain stimuli, and allodynia is pain caused by stimuli that do not normally cause pain [25]. These pathological pains are thought to be caused by plastic changes in the nature of sensory neurons in somatic sensory pathways due to inflammation or injury of peripheral tissues [22]. In general, peripheral sensitization, including increased excitability of peripheral nerve endings and chemical substance-mediated crosstalk between neurons and between neurons and glial cells in sensory ganglia due to tissue inflammation or injury, is known to trigger central sensitization, such as hyperalgesia [24-28].
3. Trigeminal Pain Transmission Pathway
In this review, we discuss the pain-relieving effect of polyphenols based on our previous in vivo research results using an animal model of trigeminal nervous system pain; thus, we first describe the trigeminal pain pathway. Pain transmission pathways are generally divided into two pathways in the trigeminal nervous system; the lateral system and the medial system [25]. From various experimental evidence to date, it is thought that the lateral pain transmission pathway conveys information on "discriminative aspects", such as "pain intensity and location" occurring in the peripheral receptive field, while the medial pain transmission pathway transmits information on the "emotional aspect" of pain, such as "pleasant or unpleasant", to a higher center [29].
First, primary sensory information, including pain, from the orofacial region (tongue, pulp, periodontal ligament, and temporomandibular joint), which is the trigeminal innervation region, is transmitted via trigeminal ganglion (TG) neurons to the trigeminal spinal nucleus caudalis (SpVc)/upper cervical dorsal horn (C1-C2) in the brainstem [24, 30]. Two types of neurons are known to respond to nociceptive stimuli at this site. One of them is the wide-dynamic range (WDR) neuron, which is thought to transmit the "pain intensity" from the peripheral receptive field to the CNS because the frequency of impulse discharge increases in proportion to stimulation intensity in both non-nociceptive and nociceptive stimulation range [24, 25]. It has been speculated that these neurons are involved in the mechanism of hyperalgesia during tissue damage and inflammation [24, 25]. The second type of neuron is the nociceptive-specific neuron which only responds to noxious stimulation of receptive fields, and thus possibly sends location-related information to higher centers [25].
In contrast, WDR neurons respond to noxious and non-noxious stimulation [24, 25]. The nociceptive information from SpVc/C1-2 is involved in the integrated processing of "discriminative aspects" of pain projected to the primary somatosensory cortex and the secondary somatosensory cortex via the medial ventral nucleus of the thalamus [31]. On the other hand, nociceptive information from the medial thalamic nucleus is transmitted via the parabrachial nucleus to the limbic amygdala, insular cortex, and anterior cingulate cortex, and is involved in the integrated processing of information on the "emotional aspect" of pain [25, 32].
4. Peripheral and Central Nociceptive Pain Transmission Mechanism
Among primary afferent nerve fibers, such as TG neurons, Aδ-fibers, which are the thinnest among myelinated fibers and have slow conduction velocities, and unmyelinated C-fibers, are involved in pain transmission [24, 25, 30]. The former is involved in the transmission of well-localized, stabbing, “fast and sharp” pain, while the latter is involved in the transmission of persistent, “slow and dull” pain that is poorly localized [23, 25]. TG neurons have the morphology of pseudo bipolar cells, and the central end of the axon makes chemical synaptic connections with secondary neurons, but the peripheral end becomes a free nerve terminal and is nociceptive [24, 25, 30]. The nociceptors play the role of energy transducers that convert exogenous noxious stimuli (thermal, cold, mechanical, chemical energy) into electrical signals [23]. As shown in (Figure 1), the conversion and transmission mechanism of sensory information in primary afferent fibers can be roughly divided into the following four general steps: (i) transduction, whereby the peripheral terminal transduces external stimuli; (ii) generation and initiation of action potentials; (iii) propagation via neurons that conduct action potentials; and (iv) transmission, whereby the central terminal forms the presynaptic element of the first synapse in the sensory terminal of the sensory pathways of the CNS [24, 33].
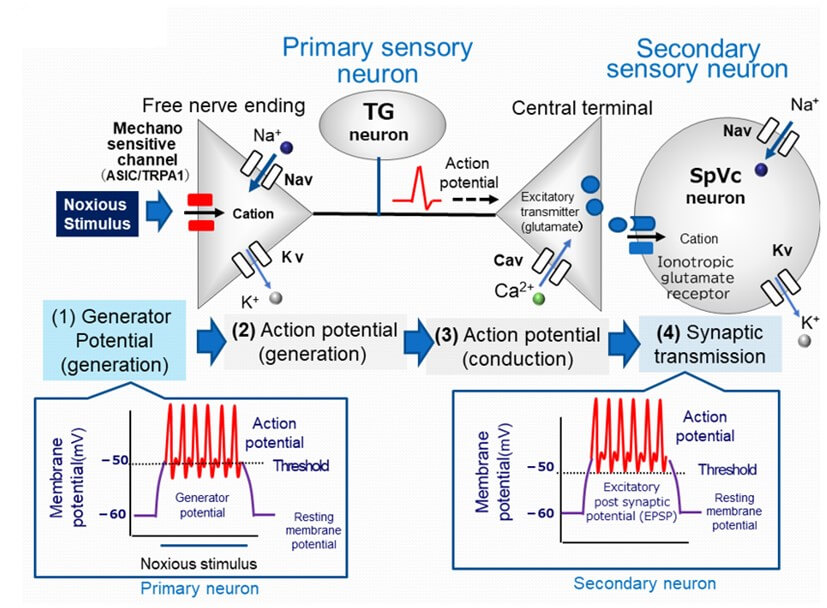
TG: Trigeminal Ganglion; Nav: Voltage-gated Sodium Channel; Kv: Voltage-gated Potassium Channel; Cav: Voltage-gated Calcium Channel; SpVc: Spinal Trigeminal Nucleus Caudalis; EPSP: Excitatory Post-Synaptic Potential; ASIC: Acid-Sensing Ion Channel; TRPA1: Transient Receptor Potential Ankyrin 1.
For example, when a nociceptive mechanical stimulus is applied to the peripheral receptive field of the skin, transient receptor potential ankyrin 1 (TRPA1) and acid-sensing ion channels (ASICs), candidate nociceptive channels that respond to nociceptive stimuli of free nerve endings, are excited and a depolarizing potential (generator potential) is generated by the influx of cations through ion channels into the cell [34-37]. This generator potential is a non-conducting local potential that functions as an analog signal with a graded amplitude of local potential depending on the intensity of the stimulus, and a conducting digital signal, the action potential (the all-or-none principle). Thus, generator potentials generated in nociceptors of primary sensory neurons are called "triggering potentials" because they trigger action potentials. When evoked potentials, generated in response to various noxious stimuli applied to free nerve terminals, exceed the threshold membrane potential (threshold for evoking action potentials), an action potential is generated by a depolarization phase due to the opening of voltage-gated Na (Nav) ion channels present on the same cell membrane and the influx of sodium ions from the outside to the inside of the cell, followed by a repolarization phase due to the outflow of potassium ions from the inside to the outside of the cell by the opening of voltage-gated K (Kv) channels [24, 33]. Nav channels expressed in nociceptive neurons are both tetrodotoxin (TTX)-sensitive (S) and TTX-resistant (R). Aδ neurons express TTX-S Nav and TTX-R Nav channels, while C-neurons mainly express TTX-R Nav channels [38].
Depending on the intensity of the noxious stimulus applied to the receptive field, the amplitude of the generator potential increases, and the firing frequency of the generated action potentials also increases [24, 25]. Action potentials generated at free nerve terminals (peripheral ends of axons) are conducted to the central end of axons through Nav and Kv channels distributed along the axons. When the action potential reaches the central end of the nerve terminal, the voltage-gated Ca (Cav) channels present at this site are opened, along with an accompanying depolarization of the nerve terminal, allowing Ca2+ to flow into the cell. An increase in the intracellular concentration of Ca2+ releases excitatory neurotransmitters (e.g., glutamate) from the presynaptic fiber into the synaptic cleft, and cations enter the cell via activation of ionotropic glutamate receptors in the secondary sensory neurons. The activation of glutamate receptor-induced cation influx generates an excitatory postsynaptic potential (EPSP), and when this potential reaches a threshold membrane potential, an action potential is generated. It is thought that the amplitude of the EPSP increases according to the amount of transmitter released, and the increase in frequency of discharge is perceived by the higher center of the CNS as information on pain intensity [24, 25].
5. Modulation of Nociceptive Transmission by Phytochemicals
5.1. Local Anesthetic Effect of Phytochemicals on Nociceptive Pain
Yu et al. previously reported that the phytochemical, resveratrol, dose-dependently suppresses the current induced by the activation of TRPA1, a candidate nociceptive mechanosensitive channel involved in the expression of nociceptive pain [18]; thus, it can be assumed that resveratrol inhibits the generator potential in sensory terminals. In addition, previous studies have shown that resveratrol dose-dependently modulates currents mediated by Nav and Kv channels in spinal dorsal root ganglion neurons, which are primary sensory neurons [11, 13]. These findings indicate that resveratrol may suppress the firing frequency of action potentials of primary sensory neurons that receive noxious stimuli and the associated generator potential. This suggests that resveratrol has the same effect as the clinically-used local anesthetic agent, lidocaine. Local anesthetics, such as lidocaine, have been reported to have side effects and complications affecting the heart, cardiovascular system, and CNS, and have the disadvantage of being less effective in inflamed sites [39]. Recently, using anesthetized rats, we demonstrated that the excitability of SpVc WDR neurons in response to non-noxious and noxious mechanical stimuli was dose-dependently and reversibly inhibited by local subcutaneous administration of resveratrol to the receptive field [40].
In addition, we also found that this inhibitory effect is almost equivalent to that of 1% lidocaine, which is a dose typically used clinically. These findings suggest that local administration of resveratrol to the peripheral receptive field inhibits TRPA1 and Nav channels and facilitate the opening of Kv channels in the peripheral free nerve endings of TG neurons, thereby decreasing the excitability of SpVc WDR neurons. This strongly suggests that resveratrol may be a substitute for local anesthetics, without any side effects on the heart and cardiovascular system [41].
Previously, Liu et al. reported that administration of the phytochemical, chlorogenic acid, facilitates Kv channel opening and inhibits ASIC channel current in acutely isolated TG neurons under in vitro conditions [42]. We then investigated the effect of topical administration of chlorogenic acid on the excitability of SpVc WDR neurons in response to non-noxious and nociceptive mechanical stimuli in anesthetized rats and found that it affected the excitability of these neurons in a dose-dependent and reversible manner. Chlorogenic acid suppresses both the triggering of generator potentials and action potentials, suggesting that a local anesthetic action may occur [43]. Moreover, in vitro experiments have demonstrated that the isoflavone, genistein, significantly suppresses both TTX-R and TTX-S Nav channel currents in acute isolated TG neurons in a concentration-dependent and reversible manner [10].
Therefore, we recently conducted an in vivo study and found that local administration of genistein into the receptive field suppressed the excitability of rat SpVc WDR neurons in a concentration-dependent manner, and the potency of 10 mM genistein had a similar inhibitory effect as 1% (37 mM) lidocaine [44]. We also found that half the amount of 1% lidocaine can be replaced with genistein. Similarly, we found that local administration of (-)-epigallocatechin -3-gallate (catechin) suppressed the excitability of nociceptive SpVc neurons, possibly by inhibiting Nav channels and facilitating the opening of Kv channels in the TG [45]. Therefore, administration of catechin as a local anesthetic may provide relief from trigeminal nociceptive pain without any side effects.
However, observation of the local anesthetic effects of dietary constituents acting on nociception has been based on changes in the excitability of nociceptive secondary neurons, and not primary afferent activity. Therefore, it still remains to be determined if local administration of such dietary constituents to rats attenuates the excitability of nociceptive primary neurons in response to mechanical stimulation in vivo. Previous studies reported in vitro conditions, quercetin inhibits Nav, Cav and activation of Kv channels in cardiac muscle [16, 19]. Recently, we found that in vivo local injection of quercetin into the peripheral receptive field suppressed the excitability of rat nociceptive primary sensory neurons in the TG, possibly via inhibition of Nav channels and opening of Kv channels in the nociceptive nerve terminals [46]. Therefore, in the absence of neuropathic and inflamed conditions, administration of the phytochemical, quercetin, as a local anesthetic may provide relief from trigeminal nociceptive pain with the smallest side effects, thus contributing to the use of CAM.
Based on the above reports, comparing the inhibitory effects of phytochemicals and lidocaine on the discharge frequency of nociceptive neurons in response to noxious stimuli, the local anesthetic action appears to be as follows: resveratrol (10 mM) = chlorogenic acid (10 mM) = isoflavones (10 mM) = (-)-epigallocatechin-3-gallate (10 mM) = quercetin (10 mM) > 1% lidocaine (37 mM). Therefore, it can be assumed that these phytochemicals are expected to have the same effect at a concentration of 1/4 that of 1% lidocaine [47]. The reason for this difference is that phytochemicals have a wider range of target molecules than lidocaine when they act on nerve terminals, and they not only inhibit Nav channels, but also inhibit mechanosensitive channels and facilitate Kv channels (Figure 2). However, further patch-clamp studies of TG neurons are needed to confirm this possibility [48, 49].
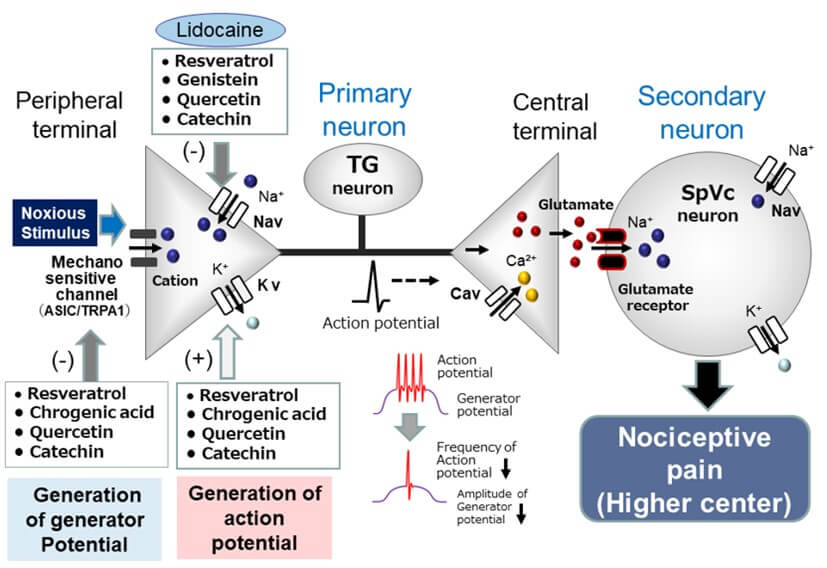
TG: Trigeminal Ganglion; Nav: Voltage-gated Sodium Channel; Kv: Voltage-gated Potassium Channel; Cav: Voltage-gated Calcium Channel; SpVc: Spinal Trigeminal Nucleus Caudalis; (+): Excitation; (-): Inhibition; ASIC: Acid-Sensing Ion Channel; TRPA1: Transient Receptor Potential Ankyrin 1; lidocaine: Local Anesthetic Agent.
5.2. Intravenous Anesthetic Effect of Phytochemicals on Nociceptive Pain
Further studies by Gao et al. have shown that resveratrol dose-dependently suppresses post-synaptic currents induced by glutamate in synaptic transmission studies using hippocampal slices in vitro [15]. In their report, glutamate n-methyl-D-aspartate (NMDA) receptors are more sensitive to resveratrol than α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA) receptors. Furthermore, resveratrol dose-dependently inhibits long-lasting-type Cav channel currents in cardiac myocytes, an excitatory cell [14]. Based on the above findings, resveratrol may inhibit glutamate receptors in the post-synaptic membrane and Cav channels in the pre-synaptic membrane, thus suppressing glutamatergic excitatory synaptic transmission in SpVc neurons, part of the glutamate-mediated synaptic transmission mechanism [50]. Recently, we investigated whether the excitability of SpVc WDR neurons in response to non-noxious and noxious mechanical stimuli was modified by intravenous administration of resveratrol in vivo [51].
As a result, we found that resveratrol dose-dependently and reversibly suppressed the firing frequency of SpVc WDR neurons responding to non-noxious and noxious mechanical stimuli. In addition, resveratrol inhibited the firing frequency of SpVc WDR neurons significantly more to noxious stimuli than to non-nociceptive stimuli. To examine the effects of resveratrol on the postsynaptic membrane, we administered resveratrol intravenously and examined the neuronal activity of these SpVc WDR neurons in response to iontophoretic administration of glutamate and NMDA using multi-barrel microelectrodes [51]. As a result, resveratrol inhibited the firing frequency induced in SpVc WDR neurons by administration of glutamate and NMDA at almost the same rate of relative inhibition. In particular, it was found to suppress the excitatory synaptic transmission mechanism via NMDA receptors [51] (Figure 3). In other words, resveratrol may have an effect equivalent to that of ketamine (an NMDA receptor blocker), and acts as an intravenous anesthetic with a high analgesic effect and fewer side effects, such as respiratory depression.

TG: Trigeminal Ganglion; PAG: Periaqueductal Grey; NRM: Nucleus Raphe Magnus; SpVc: Spinal Trigeminal Nucleus Caudalis; Glu: Glutamate; Enk: Enkephalin; AMPA: α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid; NMDA: n-methyl-D-aspartate receptor; GABA: Gamma-Aminobutyric Acid; 5HT: 5-hydroxytryptamine (serotonin); EPSP: Excitatory Post-Synaptic Potential; Nav: Voltage-gated Sodium Channel; Kv: Voltage-gated Potassium Channel; Cav: Voltage-gated Calcium Channel; (+): Excitation; (-): Inhibition; ASIC: Acid-sensing Ion Channel; TRPA1: Transient Receptor Potential Ankyrin 1; Morphine: μ-opioid receptor antagonist; ketamine: NMDA receptor antagonist; G: G Protein.
In general, μ-opioid receptors are known to exist in neurons of the periaqueductal grey (PAG), and opioids, such as morphine and encephalin, act on PAG μ-opioid receptors through activation of the descending pain inhibitory system [52, 53]. As shown in (Figure 3), the descending pain inhibitory system consists of midbrain PAG neurons and nucleus raphe magnus neurons, containing serotonergic (5HT) neurons [54, 55]. The nociceptive jaw-opening reflex is used to determine the inhibitory mechanism of pain transmission by appropriately adjusting the parameters of electrical stimulation intensity in in vitro animal experiments [56, 57]. We have also demonstrated that intravenous administration of resveratrol reversibly inhibits the nociceptive jaw-opening reflex through μ-opioid receptors under in vivo conditions [58].
In addition, 5HT3 receptor inhibition (ondansetron) and pre-administration of a GABAA receptor blocker (bicuculline) attenuates the suppression of the electrical stimulation-induced nociceptive jaw-opening reflex caused by the intravenous administration of resveratrol [59]. These experimental results indicate that intravenous administration of resveratrol activates the descending pain-inhibiting μ-opioid receptors and 5HT3 receptors under in vivo conditions, ultimately leading to GABAergic inhibition in the SpVc region. It is strongly suspected that activating and enhancing the presynaptic inhibitory mechanism mediated by μ-opioid receptors in the SpVc region inhibits nociceptive synaptic transmission [60]. Based on these facts, resveratrol may be useful as an intravenous anesthetic and analgesic, and may have similar effects as morphine, a μ-opioid receptor antagonist effective for cancer pain, and barbiturate derivatives (e.g., thiopental) and benzodiazepine derivatives (e.g., midazolam) which have sedative and sleeping effects (Figure 3).
Our extracellular electrophysiological studies in rats have found that: (i) the relative magnitude of inhibition of SpVc WDR neuronal discharge frequency caused by theanine is significantly greater for noxious than non-noxious stimulation; (ii) the mean firing frequency of SpVc WDR neurons responding to iontophoretic application of glutamate is inhibited by intravenous administration of theanine; and (iii) the mean firing frequency of SpVc WDR neurons responding to iontophoretic application of glutamate is significantly inhibited by intravenous administration of theanine [61]. Taken together, these findings suggest that acute intravenous theanine administration suppresses glutaminergic excitatory post-synaptic transmission, possibly via an NMDA receptor signaling pathway in the SpVc through convergence inputs from noxious rather than non-nonxious sensory information.
6. Modulation Mechanism of Pathological Pain by Phytochemicals
6.1. Local Anesthetic Effect of Phytochemicals on Inflammatory Pain
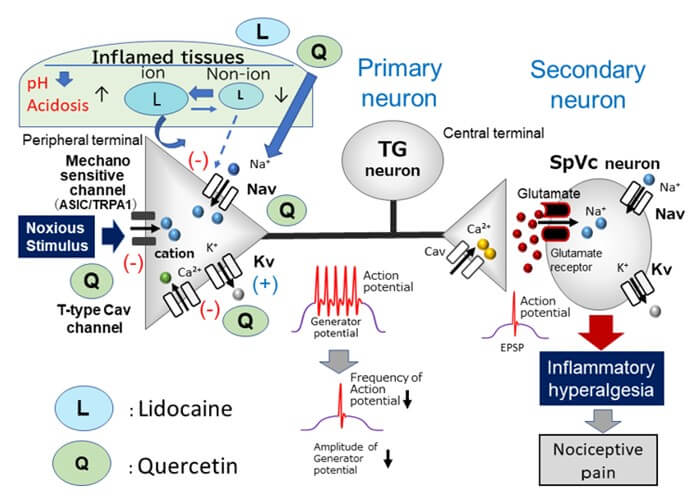
Previous studies have demonstrated that ASICs might be a candidate for mammalian cutaneous mechanoreceptors in the nerve terminals of TG neurons, along with TRPA1 [34, 35]. Moreover, the application of quercetin inhibits ASIC currents [62]. Tissue pH under inflamed conditions is less than 6.0, and low pH activates primary nociceptive afferents via ASICs [63]. Clinically, the presence of inflammation decreases local anesthetic efficacy, especially with dental anesthetics [64]. Fu et al. found that peripheral inflammation can induce the up-regulation of ASICs in TG neurons, and specific inhibitors of ASICs may have a significant analgesic effect on orofacial inflammatory pain [65]. These findings suggest that direct local administration of quercetin inhibits generator potentials, and subsequently suppresses the action potential firings of nociceptive TG neurons via inhibition of ASIC channels, inhibition of Nav channels, and opening of Kv channels in inflamed tissues.
Recently, Sashide et al. [66] reported that local injection of quercetin into the peripheral receptive field of rats suppressed the excitability of nociceptive primary sensory neurons in the TG neurons as follows: (i) the mean firing frequency of TG neurons in response to both non-noxious and noxious mechanical stimuli was reversibly inhibited by quercetin in a dose-dependent manner (1-10 mM); (ii) the mean firing frequency of inflamed TG neurons in response to mechanical stimuli was reversibly inhibited by the local anesthetic, 1% lidocaine (37 mM); and (iii) the mean magnitude of inhibition of TG neuronal discharge frequency with 1 mM quercetin was significantly greater than that of 1% lidocaine [66]. As shown in (Figure 4), these results suggest that local injection of quercetin into inflamed tissue suppresses the excitability of nociceptive primary sensory TG neurons via inhibition of ASIC channels, inhibition of Nav, and Cav channels, and opening of Kv channels. Therefore, local administration of the phytochemical, quercetin, into inflamed tissues may be a more potent local analgesic than Nav channel blockers as it inhibits the generation of both generator potentials and action potentials in nociceptive primary nerve terminals [66]. As such, quercetin contributes to the area of CAM. However, further confirmational studies, such as in vitro patch-clamp studies of dissociated fluorescently labelled TG neurons derived from the receptive field of inflammatory tissues, are needed [26, 48, 49].
6.2. Relief from Inflammatory Pain: Complete Freund's Adjuvant (CFA) Inflammation Rat Model
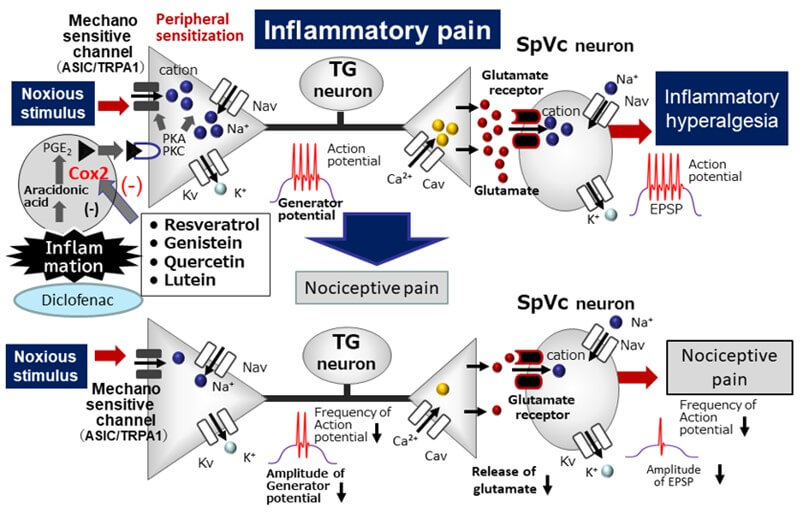
Pham-Marcou et al. reported that resveratrol regulates the cyclooxygenase-2 (Cox-2) signal cascade pathway, a synthase of PGE2, which plays a central role in the development of inflammatory pain [67]. As shown in (Figure 5), PGE2, as an inflammatory mediator, binds to G-protein-coupled E-type prostanoid receptors of primary sensory neurons distributed in inflammatory sites, and activates PKA and PKC. It also activates nociceptive ionic channels and Nav channels by phosphorylation. As a result, increased excitability (peripheral sensitization) is enhanced by an increase in the amplitude of generator potentials and a decrease in the Nav channel excitatory threshold, resulting in frequent action potentials being conducted to the CNS and reaching presynaptic terminals. High concentrations of excitatory neurotransmitters are then released via exocytosis into the synaptic cleft, binding to glutamate receptors on the postsynaptic membrane, increasing the amplitude of EPSPs, and increasing the excitability of nociceptive secondary sensory neurons (central sensitization), and pain information is transmitted to higher centers to induce hyperalgesia. Similar to non-steroidal anti-inflammatory drugs (NSAIDs), potent inhibitors of Cox-2, resveratrol suppresses inflammatory hyperalgesia via inhibiting Cox-2 activity, as evidenced by resveratrol administration attenuating pain-related behaviors induced by inflammation in animals [9].
TG: Trigeminal Ganglion; Nav: Voltage-gated Sodium Channel; Kv: Voltage-gated Potassium Channel; Cav: Voltage-gated Calcium Channel; SpVc: Spinal Trigeminal Nucleus Caudalis; ASIC: Acid-sensing Ion Channel; TRPA1: Transient Receptor Potential Ankyrin 1; (+): Excitation; (-): Inhibition; EPSP: Excitatory Post-Synaptic Potential.
Recently, we investigated whether chronic administration of resveratrol suppresses the hyperexcitability of nociceptive neurons involved in inflammatory hyperalgesia using a CFA-induced inflammation animal model. [68]. We showed that the withdrawal reflex threshold to mechanical stimulation by von Frey hairs in CFA-inflamed rats is significantly lower than in naïve rats, and systemic administration of resveratrol restores it to the level of normal animals. Two days after administration of resveratrol, central sensitivity associated with inflammation was observed in rats in the inflammation group, resulting in a decrease in the mechanical stimulus threshold, which is an index of hyperexcitability of SpVc WDR neurons, an increase in the frequency of spontaneous and evoked discharges, and an enlarged receptive field. After administration of resveratrol, all signs of central sensitization returned to normal levels.
As with resveratrol, we also reported that systemic administration of the phytochemicals, isoflavone and quercetin, restored CFA-induced inflammatory hyperalgesia and hyperexcitability of SpVc WDR neurons to the level seen in naïve rats [69, 70]. In particular, the inhibitory effect of quercetin (50 mg/kg, i.p.) on inflammatory hyperalgesia was equivalent to that of diclofenac (50 mg/kg, i.p.), a representative NSAIDs [70]. Generally, NSAIDs not only inhibit Cox-2 expressed in inflammatory sites, but also Cox-1, which is physiologically expressed in the stomach and kidneys, and thus carries the risk of side effects, such as gastrointestinal and renal disorders. Therefore, our findings suggest that chronic administration of polyphenols inhibits SpVc WDR neuron hyperexcitability through inhibition of the peripheral and Cox-2 signaling cascade pathways in nociceptive neurons and the resulting inflammatory hyperalgesia. Polyphenols, such as resveratrol, isoflavones, and quercetin, can avoid side effects and be applied as alternative treatments to NSAIDs in the prevention of inflammatory hyperalgesia (Figure 5).
TG: Trigeminal Ganglion; SpVc: Spinal Trigeminal Nucleus Caudalis; Nav: Voltage-gated Sodium Channel; Kv: Voltage-gated Potassium Channel; Cav: Voltage-gated Calcium Channel; PGE2: Prostaglandin E2; EP: E-type Prostanoid; ASIC: Acid-sensing Ion Channel; TRPA1: Transient Receptor Potential Ankyrin 1; (+): Excitation; (-): Inhibition; EPSP: Excitatory Post-Synaptic Potential; GABA: Gamma-Aminobutyric Acid; Cox-2: Cyclooxygenase-2; diclofenac: Non-Steroidal Anti-Inflammatory Drug.
This idea is also supported by our previous study [71] in which the lowered mechanical stimulation threshold in CFA-inflamed rats was returned to control levels after 3 days of daily administration of the phytochemical, lutein. Lutein administration also returned the inflammation-induced edema of the whisker pad to control levels. The increased number of Cox-2-immunoreactive cells in the whisker pads of CFA-inflamed rats was also returned to control levels by administration of lutein. The mean discharge frequency of SpVc WDR neurons to both non-noxious and noxious mechanical stimuli in CFA-inflamed rats was significantly decreased after lutein administration. Taken together, these results suggest that administration of the phytochemical, lutein, attenuates inflammatory hyperalgesia associated with the hyperexcitability of nociceptive SpVc WDR neurons via inhibition of the peripheral Cox-2 signaling cascade [71].
6.3. Relief of Ectopic Hyperalgesia: Rat Model of Orthodontic Pain
In the clinical field of dentistry, pain associated with tooth movement in orthodontic dentistry is transient in most cases, but it can be a serious problem for some patients and often causes them to avoid orthodontic treatment. In some cases, ectopic pain (pain at a site different from the original lesion), such as headache due to orthodontic tooth movement, may occur with persistent pain during mastication [72]. However, the pathological mechanism is unknown. Administration of NSAIDs is a solution to ectopic pain, but always carries the risk of stomach discomfort and other side effects. In particular, in tooth movement due to orthodontic treatment, there is concern about the decrease in osteoclasts associated with the inhibition of PGE2 synthesis by NSAIDs, and the suppression of tooth movement.
Recently, we investigated the relieving effect of resveratrol on ectopic hyperalgesia during orthodontic movement treatment in rats fitted with orthodontic appliances and induced experimental tooth movement [73]. We found that resveratrol alleviated ectopic hyperalgesia by inhibiting the hyperexcitability of pain-transmitting SpVc WDR neurons without inhibiting tooth movement. These facts strongly suggest a possible clinical application for the pain-relieving effect of phytochemicals, which could be applied to the treatment of pathological pain of the trigeminal nervous system, such as headache and temporomandibular joint pain, in the future. To date, the pathogenesis of ectopic hyperalgesia has been postulated to involve chemical-mediated crosstalk between neurons and glial cells within the TG (review, [28]). We have provided evidence that activation of sensory ganglionic satellite glial cells modulates the excitability of primary nociceptive neurons via an interlukin-1β paracrine mechanism following peripheral inflammation, and that cytokine release may be one of the important factors determining the magnitude of trigeminal inflammatory hyperalgesia [26, 27]. In the future, it will be necessary to identify the target molecules of phytochemicals involved in the crosstalk between neurons in sensory ganglia and between neurons and glial cells.
7. Concluding Remark and Perspectives
Previously, using in vitro studies, we showed that phytochemicals are involved in the activity of voltage-gated/ligand-gated ion channels and the function of neurotransmitters/receptors involved in the expression of neuronal electrical signals, including pain-transmitting neurons in the CNS and peripheral nervous system. Our neurophysiological approach in recent in vivo experiments has revealed that phytochemicals, such as resveratrol, chlorogenic acid, isoflavones, quercetin, catechin, lutein, and theanine, act on several molecular targets producing local anesthetic effects, intravenous anesthesia/analgesic effects, and inflammatory pain-alleviating effects [40, 43-46, 58, 59, 61, 66, 68-71].
In recent years, CAM has been sought out when drug treatment based on western medicine is not effective. Research that examines the possibility of pain relief using food ingredients that can avoid the various side effects of pharmaceuticals is highly important for the development of “highly safe treatment methods that do not rely on drugs.” Based on the research results of our laboratory introduced in this article, we have confirmed in vivo that phytochemicals have: (i) a local anesthetic action, (ii) an intravenous anesthetic and analgesic action, and (iii) an inflammatory pain-relieving action. In the future, advancing these studies will provide basic knowledge for the development of functional foods that are effective in relieving pain, CAM for disease treatment that does not rely on drugs, and for the development of analgesics without side effects. This would make a great contribution to medical care. Our research results introduced in this article mainly focused on verification of the “discriminative aspects” of pain (lateral system). Analysis of the involvement of phytochemicals in the "emotional aspects" of pain (medial system) is also necessary. Furthermore, the results of stuides introduced in this article will require further analysis in order to lead to clinical application.
Data Availability
No data were used for the research described in this review article.
Conflicts of Interest
None.
Funding
This study was supported by a Grant-in-Aid for Scientific Research (C) from the Japanese Society for the Promotion of Science (No.22K10232).
REFERENCES
[1] Jaya
K Rao, Kimberly Mihaliak, Kurt Kroenke, et al. “Use of complementary therapies
for arthritis among patients of rheumatologists.” Ann Intern Med, vol.
131, no. 6, pp. 409-416, 1999. View at: Publisher
Site | PubMed
[2] James
J Konvicka, Tricia A Meyer, Andrew J McDavid, et al. “Complementary/alternative
medicine use among chronic pain clinic patients.” J Perianesth Nurs,
vol. 23, no. 1, pp. 17-23, 2008. View at: Publisher Site | PubMed
[3] Eric
I Rosenberg, Inginia Genao, Ian Chen, et al. “Complementary and alternative
medicine use by primary care patients with chronic pain.” Pain Med, vol.
9, no. 8, pp. 1065-1072, 2008. View at: Publisher
Site | PubMed
[4] L
Frémont “Biological effects of resveratrol.” Life Sci, vol. 66, no. 8,
pp. 663-673, 2000. View
at: Publisher Site | PubMed
[5] Shazib
Pervaiz “Resveratrol: From grapevines to mammalian biology.” FASEB J,
vol. 17, no. 14, pp. 1975-1985, 2003. View at: Publisher
Site | PubMed
[6] Massimo D'Archivio, Carmela Filesi,
Roberta Di Benedetto, et al. “Polyphenol, dietary sources and bioavailability.”
Ann Ist Super Sanita, vol. 43, no. 4, pp. 348-361, 2007. View at: PubMed
[7] Pere Boadas-Vaello, Jose Miguel Vela,
Enrique Verdu “New pharmacological approach using polyphenols on the
physiopathology of neuropathic pain.” Curr. Drug Targets, vol. 18, no.
2, pp. 160-173, 2017. View at: Publisher
Site | PubMed
[8] Alexandra Alves-Rodrigues, Andrew
Shao “The science behind lutein.” Toxicol Lett, vol. 150, no. 1, pp.
57-83, 2004. View at: Publisher
Site | PubMed
[9] M Gentilli, J X Mazoit, H Bouaziz, et
al. “Resveratrol decreases hyperalgesia induced by carrageenan in the rat hind
paw.” Life Sci, vol. 68, no. 11, pp. 1317-1321, 2001. View at: Publisher Site | PubMed
[10]
Lieju
Liu, Tianming Yang, S A Simon “The protein tyrosine kinase inhibitor,
genistein, decreases excitability of nociceptive neurons.” Pain, vol.
112, no. 1-2, pp. 131-141, 2004. View at: Publisher Site | PubMed
[11]
Zhao-Bing
Gao, Guo-Yuan Hu “Trans-resveratrol, a red wine ingredient, inhibits
voltage-activated potassium currents in rat hippocampal neurons.” Brain Res,
vol. 1056, no. 1, pp. 68-75, 2005. View at: Publisher Site | PubMed
[12]
Han-Seong
Jeong, Yo-Sik Kim, Jong-Seong Park “Modulation of neuronal activity by EGCG.” Brain
Res, vol. 1047, no. 2, pp. 267-279, 2005. View at: Publisher Site | PubMed
[13]
Hong
Im Kim, Tae Hoon Kim, Jin-Ho Song “Resveratrol inhibits Na+ currents
in rat dorsal root ganglion neurons.” Brain Res, vol. 1045, no. 1-2, pp.
134-141, 2005. View at: Publisher
Site | PubMed
[14]
Reginald
Liew, Mark A Stagg, Kenneth T MacLeod, et al. “The red wine, resveratrol,
exerts acute direct action on gunia-pig ventricular myocytes.” Eur J
Pharmacol, vol. 519, no. 1-2, pp. 1-8, 2005. View at: Publisher Site | PubMed
[15]
Zhao-Bing
Gao, Xue-Qin Chen, Guo-Yuan Hu “Inhibition of excitatory synaptic transmission
by trans-resveratrol in rat hippocampus.” Brain Res, vol. 1111, no. 1,
pp. 41-47, 2006. View at: Publisher Site | PubMed
[16]
Catriona
H R Wallace, Istvan Baczkó, Brian K Jones, et al. “Inhibition of cardiac
voltages-gated sodium channels by grape polyphenols.” Br J Pharmacol,
vol. 149, no. 6, pp. 657-665, 2006. View at: Publisher Site | PubMed
[17]
Tae
Hoon Kim, Jae-Min Lim, Sung Su Kim, et al. “Effects of
(-)-epigallocatechin-3-gallate on Na(+) currents in rat dorsal root ganglion
neurons.” Eur J Pharmacol, vol. 604, no. 1-3, pp. 20-26, 2009. View at: Publisher Site | PubMed
[18]
Lina
Yu, Shenglan Wang, Yoko Kogure, et al. “Modulation
of TRP channels by resveratrol and other stilbenoids.” Mol Pain,
vol. 9, pp. 3, 2013. View at: Publisher
Site | PubMed
[19]
Xiaomin
Hou, Yu Liu, Longgang Niu, et al. “Enhancement of voltage-gated K+ channels and
depression of voltage-gated Ca2+ channels are involved in quercetin-induced
vasorelaxation in rat coronary artery.” Planta Med, vol. 80, no. 6, pp.
465-472, 2014. View at: Publisher
Site | PubMed
[20]
Ichrak
Drissi, William Aidan Woods, Christopher Geoffrey Woods “Understanding the
genetic basis of congenital insensitivity to pain.” Br Med Bull, vol.
133, no. 1, pp. 65-78, 2020. View at: Publisher Site | PubMed
[21] Hong
Cao, Yu-Qiu Zhang “Spinal glial activation contributes to pathological pain
states.” Neurosci. Biobehav Rev, vol. 32, no. 5, pp. 972-983,
2008. View at: Publisher Site | PubMed
[22] Joachim
Scholz, Clifford J Woolf “Can we conquer pain?” Nat Neurosci, vol. 5
Suppl, pp. 1062-1067, 2002. View at: Publisher Site | PubMed
[23]
Cervero
F “Pain theories.” in: Basbaum, A.I., Bushnell, M.C. (Eds.), Science of Pain.
Elsevier, Amsterdam, pp. 5-10, 2013.
[24] Mamoru
Takeda, Shigeji Matsumoto, Barry J. Sessle, et al. “Peripheral and central
mechanisms of trigeminal neuropathic and inflammatory pain.” Journal of Oral
Biosciences, vol. 53, no. 4, pp. 318-329, 2011. View at: Publisher Site
[25]
Koichi
Iwata, Mamoru Takeda, Seog Bae Oh, et al. Neurophysiology of orofacial pain, in: Farah, C.S.,
Balasubramaniam, R., McCullough, M.J. (Eds.), Contemporary Oral Medicine.
Springer International, Zurich, pp. 1749-1773, 2017.
[26]
Mamoru
Takeda, Takeshi Tanimoto, Jun Kadoi, et al. “Enhanced excitability of
nociceptive trigeminal ganglion neurons by satellite glial cytokine following
peripheral inflammation.” Pain, vol. 129, no. 1-2, pp. 155-166, 2007.
View at: Publisher
Site | PubMed
[27]
Mamoru
Takeda, Masayuki Takahashi, Shigeji Matsumoto “Contribution of activated
interleukin receptors in trigeminal ganglion neurons to hyperalgesia via
satellite glia interleukin-1β paracrine mechanism.” Brain Behav Immun, vol. 22,
no. 7, pp. 1016-1023, 2008. View at: Publisher Site | PubMed
[28]
Mamoru Takeda, Masayuki Takahashi, Shigeji Matsumoto
“Contribution of the activation of satellite glia in sensory ganglia to
pathological pain.” Neurosci Biobehav Rev, vol. 33, no.6, pp. 784-792,
2009. View at: Publisher
Site | PubMed
[29] Ronald
Dubner “The effect of behavioral state on the sensory processing of nociceptive
and non-nociceptive information.” Prog Brain Res, vol. 77, pp. 213-218,
1988. View at: Publisher Site | PubMed
[30]
Barry John Sessle “Acute and chronic craniofacial
pain: Brainstem mechanisms of nociceptive transmission and neuroplasticity, and
their clinical correlates.” Crit Rev Oral Biol Med, vol. 11, no. 1, pp.
57-91, 2000. View at: Publisher
Site | PubMed
[31]
Khulood
M Al-Khater, Andrew J Todd “Collateral projections of neurons in laminae I,
III, and IV of rat spinal cord to thalamus, periaqueductal gray matter, and
lateral parabrachial area.” J Comp Neurol, vol. 515, no. 6, pp. 629-646,
2009. View at: Publisher
Site | PubMed
[32]
Shin-Ichi
Ito “Possible representation of somatic pain in the rat insular visceral
sensory cortex: a field potential study.” Neurosci Lett, vol. 241, no.
2-3, pp. 171-174, 1998. View at: Publisher Site | PubMed
[33] Andrea
M Harriott, Michael S Gold “Contribution of primary afferent channels to
neuropathic pain.” Curr Pain Headache Rep, vol. 13, no. 3, pp. 197-207,
2009. View at: Publisher Site | PubMed
[34]
Margaret
P Price, Sabrina L McIlwrath, Jinghui Xie, et al. “The DRASIC cation channel contributes to the detection of cutaneous touch
and acid stimuli in mice.” Neurons, vol. 32, no. 6, pp. 1071-1083, 2001.
View at: Publisher
Site | PubMed
[35]
Kelvin
Y Kwan, Joshua M Glazer, David P Corey, et al. “TRPA1 modulates mechanotransduction in cutaneous sensory neurons.”
J Neurosci, vol. 29, no. 15, pp. 4808-4819, 2009. View at: Publisher Site | PubMed
[36]
Jasenka
Borzan, Chengshui Zhao, Richard A Meyer, et al. “A role for acid-sensing ion
channel 3, but not acid-sensing ion channels 2, in sensing dynamic mechanical
stimuli.” Anesthesiology, vol. 113, no. 3, pp. 647-654, 2010. View at: Publisher Site | PubMed
[37]
Sinyoung
Kang, Jun Ho Jang, Margaret P Price, et al. “Simultaneous disruption of mouse ASIC1a,
ASIC2 and ASIC3 genes enhances cutaneous mechanosensitivity.” PLoS
One, vol. 7, no. 4, pp. e35225, 2012. View at: Publisher Site | PubMed
[38]
A
N Akopian, L Sivilotti, J N Wood “A tetrodotoxin-resistant voltage-gated sodium
channel expressed by sensory neurons.” Nature, vol. 379, no. 6562, pp.
257-262, 1996. View at: Publisher
Site | PubMed
[39]
Miller
R.D. “Local anesthetics.” in: Katzung, B.G. (Ed), Basic and Clinical
Pharmacology. Lange Medical Books/McGraw-Hill, New York, pp. 425-433, 1996.
[40]
Yoshihito
Shimazu, Eri Shibuya, Shiori Takehana, et al. “Local administration of
resveratrol inhibits excitability of nociceptive wide-dynamic range neurons in
rat trigeminal spinal nucleus caudalis.” Brain Res Bull, vol. 124, pp.
262-268, 2016. View at: Publisher
Site | PubMed
[41] Mamoru
Takeda M., Shiori Takehana, Yoshihito Shimazu “The polyphenolic compound
resveratrol attenuates pain: Neurophysiological mechanisms.” in: Watson, R.R.,
Preedy, V.R., Zibadi, S. (Eds), Polyphenol: Mechanisms of Action in Human
Health and Disease. Academic Press, London, pp. 237-247, 2018.
[42]
Fei
Liu, Xiao-Wen Lu, Yu-Jiao Zhang, et al. “Effect of chlorogenic acid on
voltage-gated potassium channels of trigeminal ganglion neurons in an inflammatory
environment.” Brain Res Bull, vol. 127, pp. 119-125, 2016. View at: Publisher
Site | PubMed
[43]
Kaede Kakita, Hirona Tsubouchi, Mayu Adachi,
et al. “Local subcutaneous injection of chlorogenic acid inhibits the
nociceptive trigeminal spinal nucleus caudalis neurons in rats.” Neurosci
Res, vol. 134, pp. 49-55, 2018. View at: Publisher Site | PubMed
[44]
Manaka
Yamaguchi, Rina Kinouchi, Shiori Morizumi, et al. “Local administration of
genistein as a local anesthetic agent inhibits the trigeminal nociceptive
neuronal activity in rats.” Brain Res Bull, vol. 172, pp. 120-128, 2021.
View at: Publisher
Site | PubMed
[45]
Mizuho
Uchino, Yukito Sashide, Mamoru Takeda “Suppression of the Excitability of Rat
Nociceptive Secondary Sensory Neurons following Local Administration of the
Phytochemical, (-)-Epigallocatechin-3-gallate.” Brain Res, vol. 1813,
pp. 148426, 2023. View at: Publisher Site | PubMed
[46]
Ryou
Toyota, Haruka Ito, Yukito Sashide, et al. “Suppression of the excitability of
rat nociceptive primary sensory neurons following local administration of the
phytochemical quercetin.” J Pain, vol. 24, no. 3, pp. 540-549, 2023.
View at: Publisher
Site | PubMed
[47] Mamoru
Takeda, Yoshihito Shimazu “Dietary constituents act as local anesthetic agents:
neurophysiological mechanism of nociceptive pain (Chapter 40).” in: Rajendram,
R., Patel, V., Preedy, V.R. (Eds), The Neuroscience of Pain, Anesthetics and Analgesics; Volume 2:
Treatments, Mechanisms, and Adverse Reactions of Anesthetics and Analgesics.
Academic Press, Cambridge, pp. 473-485,
2021.
[48]
Mamoru Takeda, Takeshi Tanimoto,
Mizuho Ikeda, et al.
“Enhanced excitability of rat trigeminal root ganglion neurons via decrease in
A-type potassium currents following temporomandibular joint inflammation.” Neuroscience,
vol. 138, no. 2, pp. 621-630, 2006. View at: Publisher
Site | PubMed
[49]
Kazuharu
Nakagawa, Mamoru Takeda, Yoshiyuki Tsuboi, et al. “Alternation of primary
afferent activity following inferior alveolar nerve transection in rats.” Mol
Pain, vol. 6, pp. 9, 2010. View at: Publisher Site | PubMed
[50]
Shiori
Takehana, Kenta Sekiguchi, Maki Inoue, et al. “Systemic administration of
resveratrol suppress the nociceptive neuronal activity of spinal trigeminal
nucleus caudalis in rats.” Brain Res Bull, vol. 120, pp. 117-122, 2016.
View at: Publisher
Site | PubMed
[51] Shiori Takehana, Yoshiko Kubota,
Nobuo Uotsu, et al. “The dietary constituent resveratrol suppresses nociceptive
transmission via NMDA receptor.” Mol Pain, vol. 13, pp.
1744806917697010, 2017.
View at: Publisher
Site | PubMed
[52]
Gebhart, G.F., Alan Randich “Brain stem modulation of
nociception.” In: Klem WR; Vertes RP eds. Brain stem mechanisms of behavior New
York, Wiley-Intersciences Publication, pp. 315-352, 1990.
[53]
B
Chieng 1, M J Christie “Hyperpolization by opioids acting on μ-receptors of a
subpopulation of rat periaqueductal grey neurons in vitro.” Br J
Pharmacol, vol. 113, no. 1, pp. 121-128, 1994. View at: Publisher
Site | PubMed
[54]
Takeshi
Tanimoto, Mamoru Takeda, Toshimi Nishikawa, et al. “The role of 5-HT3
receptors in the vagal afferent activation-induced of C1 spinal neurons
projected from tooth-pulp in the rat.” J Pharmacol Exp Ther, vol. 311,
no. 2, pp. 803-810, 2004. View at: Publisher Site | PubMed
[55]
Katsuo
Oshima, Mamoru Takeda, Takeshi Tanimoto, et al. “Tooth-pulp-evoked rostral
spinal trigeminal nucleus neuron activity is suppressed by conditioning sciatic
nerve stimulation in the rats: possible role of 5HT3 receptor
mediated GABA ergic inhibition.” Brain Res Bull, vol. 65, no. 1,
pp. 31-40, 2005. View at: Publisher
Site | PubMed
[56]
Peggy Mason, Andrew Strassman,
Raymond Maciewicz “Is
the jaw-opening reflex a valid model of pain?” Brain Res, vol. 357, no. 2,
pp. 137-146, 1985. View at: Publisher Site | PubMed
[57]
Mamoru Takeda, Takeshi Tanimoto,
Kouei Ojima, et al.
“Suppressive effect of vagal afferents on the activity of trigeminal neurons
related to jaw-opening reflex in rats: involvement of endogenous opioid
system.” Brain Res Bull, vol. 47, no. 1, pp. 49-56, 1998. View at: Publisher Site | PubMed
[58]
Shota Kokuba, Shiori Takehana, Katsuo Oshima,
et al. “Systemic administration of the dietary constituent resveratrol inhibits
the nociceptive jaw-opening reflex in rats via the endogenous opioid system.” Neurosci Res, vol. 119, pp. 1-6, 2017. View at: Publisher Site | PubMed
[59]
Kounosuke
Hirata, Yuto Nishiki, Ryosuke Goto, et al. “Resveratrol suppresses nociceptive
jaw-opening reflex via 5HT3 receptor-mediated GABAergic inhibition.”
Neurosci Res, vol. 160, pp. 25-31, 2020. View at: Publisher Site | PubMed
[60]
Mamoru Takeda, Takeshi Tanimoto,
Mizuho Ikeda, et al.
“Opioidergic modulation of excitability of rat trigeminal root ganglion neurons
projection to the superficial layer of cervical dorsal horn.” Neuroscience,
vol. 125, no. 4, pp. 995-1008, 2004. View at: Publisher
Site | PubMed
[61]
Shiori
Takehana, Yoshiko Kubota, Nobuo Uotsu, et al. “Acute intravenous administration
of dietary constituent theanine suppresses noxious neuronal synaptic
transmission of trigeminal spinal nucleus caudalis in rats.” Brain Res Bull,
vol. 131, pp. 70-77, 2017. View at: Publisher
Site | PubMed
[62]
Mohona
Mukhopadhyay, Anurag Singh, S Sachchidanand, et al. “Quercetin inhibits
acid-sensing ion channels through a putative binding site in the central
vestibular region.” Neuroscience, vol. 348, pp. 264-272, 2017. View at: Publisher
Site | PubMed
[63]
A
Punnia-Moorthy “Evaluation of pH changes in inflammation of the subcutaneous
air pouch lining in the rat, induced by carrageenan, dextran and Staphylococcus
aureus.” J Oral Pathol, vol. 16, no. 1, pp. 36-44, 1987. View at: Publisher
Site | PubMed
[64]
Araceli
Boronat López, Miguel Peñarrocha Diago “Failure of locoregional anesthesia in
dental practice. Review of the literature.” Med Oral Patol Oral Cir Bucal,
vol. 11, no. 6, pp. E510-E513, 2006. View at: PubMed
[65]
Hui
Fu, Peng Fang, Hai-Yun Zhou, et al. “Acid-sensing ion channels in trigeminal
ganglion neurons innervating the orofacial region contribute to orofacial
inflammatory pain.” Clin Exp Pharmacol Physiol, vol. 43, no. 2, pp.
193-202, 2016. View at: Publisher
Site | PubMed
[66]
Yukito
Sashide, Ryou Toyota, Mamoru Takeda “Local administration of the phytochemical,
quercetin, attenuates the hyperexcitability of rat nociceptive primary sensory
neurons following inflammation comparable to lidocaine.” J Pain, vol.
25, no. 3, pp. 755-765, 2024. View at: Publisher Site | PubMed
[67]
Thi
Aurore Pham-Marcou, Hélène Beloeil, Xueging Sun, et al. “Antinociceptive effect
of resveratrol in carrageenun-evoked hyperalgesia in rats: prolonged effect
related to COX-2 expression impairment.” Pain, vol. 140, no. 2, pp.
274-283, 2008. View at: Publisher
Site | PubMed
[68]
Kenta
Sekiguchi, Shiori Takehana, Eri Shibuya, et al. “Resveratrol attenuates
inflammation-induced hyperexcitability of trigeminal spinal nucleus caudalis
neurons associated with hyperalgesia in rats.” Mol Pain, vol. 12, pp. 1744806916643082,
2016. View at: Publisher Site | PubMed
[69]
Shuho
Arakawa, Mogami Inoue, Rina Kinouchi, et al. “Dietary constituents genistein
inhibits the hyperexcitability of trigeminal nociceptive neurons associated
with mechanical hyperalgesia following orofacial inflammation.” J Oral
Biosci, vol. 61, no. 4, pp. 215-220, 2019. View at: Publisher Site | PubMed
[70]
Haruka
Itou, Ryou Toyota, Mamoru Takeda “Phytochemical quercetin alleviates
hyperexcitability of trigeminal nociceptive neurons associated with
inflammatory hyperalgesia comparable to NSAIDs.” Mol Pain, vol. 18, pp.
17448069221108971, 2022. View at: Publisher Site | PubMed
[71]
Yumiko Syoji, Ryota Kobayashi, Nako Miyamura, et
al. “Suppression of hyperexcitability of trigeminal nociceptive neurons
associated with inflammatory hyperalgesia following systemic administration of
lutein via inhibition of cyclooxygenase-2 cascade signaling.” J Inflamm
(Lond), vol. 15, pp. 24, 2018. View at: Publisher
Site | PubMed
[72] Marianne Bergius, Ulf Berggren, Stavros Kiliaridis “Experience of pain during an orthodontic procedure.” Eur J Oral Sci, vol. 110, no. 2, pp. 92-98, 2002. View at: Publisher Site | PubMed
[73] Nao Okubo, Haruna Ishikawa, Rena Sano, et al. “Effect of resveratrol on the hyperexcitability of nociceptive neurons associated with ectopic hyperalgesia induced by experimental tooth movement.” Eur J Oral Sci, vol. 128, no. 4, pp. 275-283, 2020. View at: Publisher Site | PubMed